Dynamic Surgical Guidance to Facilitate Dental Implant Placement
- Nov 30, 2020
- 6 min read
Updated: Jan 21, 2021
INTRODUCTION:
The long-term success of dental implant surgery is dependent, in part, on accurate planning and placement of the implant.1 Currently, there are many digital planning systems available to aid the clinician in pre-operative treatment planning, although the main challenge with these planning systems is to accurately transfer the digital plan to the clinical situation. Most systems involve taking a cone beam computed tomography (CBCT) or other three-dimensional scan of the patient, and then digitally placing implants using a software program.
Traditionally, static surgical guides are used to relate the digital planned position of the implants to the clinical situation. However, there are several drawbacks to static surgical guides. Specically, the surgical guide cannot be modied intraoperatively to adapt to chairside decisions that result in changes to the clinical plan. Furthermore, static guides are typically designed over the surgical site, and so there is some impediment to the visualization of the surgical field. Finally, the static guides have small but signicant distortions associated with them, resulting in an accuracy of implant placement that varies widely. Studies have reported wide ranges of deviations in implant placement relative to the planned position in both apico-coronal and angular dimensions for most commercially available systems.2-6 Inaccurate implant placement can result in short-term complications, such as damage to adjacent vital structures, as well as a long-term increase in implant failure.7-9.
A new technology to address these drawbacks is dynamic surgical guidance.10-12 Dynamic surgical guidance technology involves a computerized navigational system intended to provide assistance in both the planning (pre-operative) and the surgical (intra-operative) phases of dental implantation surgery. Dynamic surgical guidance provides two main modes of operation: preoperative case planning and intraoperative surgical treatment. In the preoperative phase, the system is first used to plan the dental procedure including the planned implant location within the CBCT image. During the planning phase, the clinician can select the implant system for each surgical site. Case planning can be done prior to the day of surgery, in which case the treatment plan can be saved into the case management database or, alternatively, the case can be planned immediately prior to surgery.
CASE PRESENTATION
A 72-year-old Caucasian female presented to Cityview Periodontal Center with a missing #46. The patient’s chief complaint was the “desire to replace her missing tooth”. A comprehensive examination was conducted, including an intraoral examination, digital impressions, and radiographs (Figs. 1 & 2) . The radiographs identified that the inferior alveolar nerve was in close proximity to the planned location of the implant.

TREATMENT:
Multiple treatment options were presented to the patient, including placing two implants to replace #46 and #47. The patient chose to only replace #46 at this time. Due to the challenging nature of the case, it was decided to use dynamic surgical guidance for both the implant planning and surgical phases.
IMAGING PHASE
An imaging stent with radiopaque teeth was fabricated from the digital impression (Fig. 3) . In case the patient chose to replace #37 and #47 in the future, these teeth were also added to the stent. Then, a plastic marker that also serves to hold the patient tracker (called a fiducial) was added to the imaging stent, and a cone beam computed tomography (CBCT) scan taken with the imaging stent/fiducial in place (Fig. 4) .

IMPLANT PLANNING PHASE
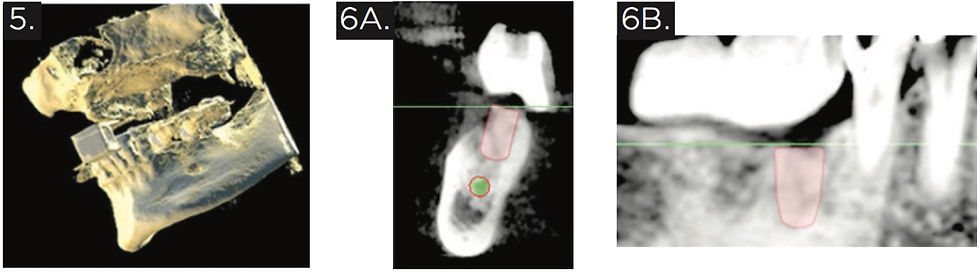
The CBCT images, with the radiopaque prosthetic plan visible in the scan, were uploaded into an implant planning software program associated with the dynamic surgical guidance system. Then, the ideal implant size and position was planned using the software, respecting the anatomical limitations of the area (Fig. 5-6) . The digital plan for the final implant position was confirmed and the patient was prepared for surgery.
PRE-SURGICAL SETUP PHASE
Immediately prior to surgery, the patient took 300mg clindamycin orally, and rinsed with 0.12% chlorhexidine rinse for one minute. The imaging stent was modied to eliminate the portion of the stent in the surgical area, and the tracking arm was attached (Fig. 7). Both the tracking arm and the handpiece (Fig. 8) contain black marking dots that can be identied optically by tracking cameras that attach to the overhead light (Fig. 9) . This setup constitutes the basis for the dynamic surgical guidance system, which is able to identify the drill position relative to the patient position intraoperatively.

SURGICAL PHASE
A full thickness flap was raised to the mucogingival junction. Then, the stent with the tracking arm was secured onto the patient’s anterior and left posterior teeth, and stability of the stent was veried. An osteotomy was prepared in #46 position using the recommended drills and sequence. The dynamic surgical guidance system was used throughout the surgical phase to identify the position of the drills within the patient’s anatomy using the CBCT scan images, and viewed on a screen behind the patient (Figs. 10 & 11). A Strauman SLActive 4.8 mm WN x 8 mm implant was placed successfully according to the dynamic surgical guidance plan, with adequate distance (>2 mm) from the apex of the implant to the inferior alveolar nerve canal. A 3mm healing abutment was placed and the ap sutured using 4-0 vicryl sutures. Final clinical photographs and a periapical radiograph were taken (Figs. 12 & 13) .


RESTORATIVE PHASE
After approximately three months healing, the stability of the implant was tested using a reverse torque test. A peri-apical radiograph veried that the bone levels around the implant remained acceptable and that the implant was ready to restore (Fig. 14) . Digital impressions were taken using a Straumann Monobody scan body and the iTero digital scanner. A direct screw-retained #46 implant crown was made (Fig. 15) . The abutment screw was torqued to 35 N-cm (Fig. 16) . The occlusal access hole was filled with a Teflon tape spacer and an occlusal composite restoration (Fig. 17) .

CONCLUSION
Dynamic surgical guidance is a tool available to implant surgeons that has the potential to increase predictability of implant placement. The ability to visualize the dental implant drills within a three-dimensional view of the patient’s anatomy provides a major advantage in dental implant surgical technology. In this case report, dynamic surgical guidance was used to ensure safe, accurate, and efficient planning and placement of a dental implant in the posterior mandible in a challenging anatomic situation.
BIOGRAPHY
Jill Bashutski is an Adjunct Clinical Assistant Professor at the University of Michigan where she previously served as Acting Director of Graduate Periodontics and Director of Undergraduate Periodontics. Dr. Bashutski obtained her dental degree from Western University in London, Ontario. She later obtained her Certificate in Periodontology, Master’s of Science in Dentistry, and Lazzara Fellowship in Advanced Implant Therapy at the University of Michigan. She serves as a senior editorial review board member for Implant Dentistry and the Journal of Oral and Maxillofacial Research and has authored over 30 articles and five book chapters on periodontics and implant dentistry, including a first-authored paper in the prestigious New England Journal of Medicine. In 2015, she received the Junior Alumni of Distinction Award from Western University for her contributions to research and teaching. Dr. Bashutski also works in private practice in Regina, SK, Canada. She can be reached at jillbashutski@gmail.com.
REFERENCES
Azari A, Nikzad S. Computer-assisted implantology: historical background and potential outcomes – a review. Int J Med Robotics Comput Assist Surg. 2008 Jun;4(2):95-104. doi: 10.1002/rcs.188
Wittwer G, Adeyemo WL, Schicho K, Birkfellner W, Enislidis G. Prospective randomized clinical comparison of 2 dental implant navigation systems. Int J Oral Maxillofac Implants 2007;22:785-790
Valente F, Schiroli G, Sbrenna A. Accuracy of computer-aided oral implant surgery: a clinical and radiographic study. Int J Oral Maxillofac Implants 2009;24:234-242.
Van Assche N, van Steenberghe D, Guerrero ME, et al. Accuracy of implant placement based on pre-surgical planning of three-dimensional cone-beam images: a pilot study. J Clin Periodontol 2007;34:816-821.
Ozan O, Turkyilmaz I, Ersoy AE, McGlumphy EA, Rosenstiel SF. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement. J Oral Maxillofac Surg 2009;67:394-401.
Van Assche N, van Steenberghe D, Quirynen M, Jacobs R. Accuracy assessment of computer-assisted flapless implant placement in partial edentulism. J Clin Periodontol;37:398-403.
de Almeida EO, Pellizzer EP, Goiatto MC, et al. Computer-guided surgery in implantology: review of basic concepts. J Craniofac Surg 2010;21:1917-1921.
Greenstein G, Cavallaro J, Romanos G, Tarnow D. Clinical recommendations for avoiding and managing surgical complications associated with implant dentistry: a review. J Periodontol 2008;79:1317-132
Greenstein G, Cavallaro J, Tarnow D. Practical application of anatomy for the dental implant surgeon. J Periodontol 2008;79:1833-1846.
Nijmeh AD, Goodger NM, Hawkes D, Edwards PJ, McGurk M. Image-guided navigation in oral and maxillofacial surgery. Br J Oral Maxillofac Surg. 2005 Aug;43(4):294-302.
Bouchard C, Magill JC, Nikonovskly V, Byl M, Murphy BA, Kaban LB, Troulis MJ. Osteomark: a surgical navigation system for oral and maxillofacial surgery. Int J Oral Maxillofac Surg. 2012 Feb;41(2):265- 270. doi: 10.1016/j.ijom.2011.10.017.
Jung RE, Schneider D, Ganeles J, Wismeijer D, Zwahlen M, Hämmerle CHF, Tahmaseb A. Computer technology applications in surgical implant dentistry: a systematic review. Int J Oral Maxillofac Implants. 2009;24(Suppl):92-109.
Inliant Dental Navigation System – Design History File. Compilation of internal technical development documentation including product description, design documents, test protocols and reports.
Inliant Dental Navigation System – Risk Management and Usability Engineering File. Compilation of internal product risk management documentation including risk analyses and risk management reports.
Inliant Clinical – User Manual. Internal Document No. PD-IFU-00049, Rev 2, Sept. 2014.
Ruppin J, Popovic A, Strauss M, Spüntrup E, Steiner A, Stoll C. Evaluation of the accuracy of three different computer- aided surgery systems in dental implantology: optical tracking vs. stereolithographic splint systems. Clin Oral Implants Res. 2008 Jul;19(7):709-716. doi: 10.1111/j.1600-0501.2007.01430.x
Hoffmann J, Westendorff C, Gomez-Roman G, Reinert S. Accuracy of navigation- guided socket drilling before implant installation compared to the conventional free-hand method in a synthetic edentulous lower jaw model. Clin Oral Implants Res. 2005 Oct;16(5):609-614.
Wittwer G, Adeyemo WL, Schicho K, Gigovic N, Turhani D, Enislidis G. Computer-guided flapless transmucosal implant placement in the mandible: a new combination of two innovative techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Jun;101(6):718- 723. doi: 10.1016/j.tripleo.2005.10.047
Download a printable PDF



Excellent, highly informative case study! The explanation of dynamic surgical guidance and its real-world application makes complex implant technology easy to understand while highlighting the importance of precision and patient safety. Educational content like this builds confidence and trust exactly what families value when choosing a knowledgeable Kids Dentist in Corona, CA.
Orange Dental is a trusted Dental Company in Toronto, providing top-quality care with expert dentists and a patient-first approach for a healthy smile.